What Is OSHA’s Respiratory Protection Standard?

If you’ve ever handed a worker a respirator and sent them off to do a job, you’ve already started down the road that 29 CFR 1910.134 is designed to govern. OSHA’s respiratory protection standard isn’t just a regulatory checkbox — it’s a comprehensive framework that tells employers exactly what they’re responsible for when workers face airborne hazards on the job. And the scope of that responsibility goes well beyond “make sure people are wearing masks.”
Here, we break down what the standard actually requires, what it means in practice, and why the pieces of the program matter even when inspectors aren’t around.
If you are looking for training for your employees on respiratory protection, our full-length training package is what you are looking for.
What 29 CFR 1910.134 Actually Covers
OSHA’s respiratory protection standard applies to any general industry employer where workers are exposed to airborne contaminants — particulates, gases, vapors, biological agents, or oxygen-deficient atmospheres — at levels that require respiratory protection. A companion standard, 29 CFR 1926.103, covers construction, but it directly references 1910.134 for most of its requirements, so the two are effectively aligned.
The standard sets minimum requirements for a written respiratory protection program, respirator selection, medical evaluations, fit testing, training, maintenance, and recordkeeping. It also draws an important distinction between required respirator use — where OSHA standards or air monitoring data indicate respiratory protection is mandatory — and voluntary use, where workers choose to wear respirators even when exposure levels don’t technically demand it. Both situations carry different obligations under the standard, and employers sometimes get tripped up assuming that voluntary use requires no program at all. For voluntary use of anything more protective than a filtering facepiece, a written program is still required.
The Written Respiratory Protection Program
The foundation of the standard is a written program — a site-specific document that spells out how your organization selects, uses, cleans, maintains, and replaces respirators. It has to be tailored to your workplace. A boilerplate program downloaded from the internet and never modified doesn’t satisfy the requirement, and more importantly, it won’t protect anyone.
The written program must designate a program administrator who is knowledgeable about the standard and qualified to make decisions about respirator selection and program management. This doesn’t have to be a full-time role, but it does have to be a real one. I’ve been in facilities where the “program administrator” couldn’t identify the difference between an organic vapor cartridge and a particulate filter — that’s a liability that starts at the top.
At a minimum, your written program should address: procedures for selecting respirators, medical evaluation procedures, fit testing procedures, procedures for proper use (including in special situations like beards or temperature extremes), procedures for maintenance and storage, procedures for regularly evaluating program effectiveness, and training requirements.
Medical Evaluations: The Step Most Employers Skip
Before any employee is required to wear a respirator, OSHA requires a medical evaluation to ensure the worker is physically able to do so. Wearing a respirator increases breathing resistance and can put strain on the cardiovascular system — it’s not appropriate for everyone.

The evaluation is done using a confidential medical questionnaire (the OSHA 1910.134 Appendix C form) administered by a physician or licensed health care professional (PLHCP). The worker fills it out, the PLHCP reviews it, and the employer receives a written recommendation: cleared to wear, cleared with restrictions, or not cleared. Employers never see the completed questionnaire — only the recommendation.
Medical evaluations are required before fit testing, before initial use, and when conditions change that could affect the worker’s ability to use a respirator safely. I’ve trained workers who had undiagnosed cardiac conditions that came to light during this process. The medical evaluation isn’t red tape — in some cases, it’s the thing that prompts someone to get care they didn’t know they needed.
Fit Testing: It’s Not Just About Comfort
Once a worker has medical clearance, the respirator has to be fit tested. A tight-fitting facepiece — whether it’s a disposable N95 or a full-face elastomeric respirator — can only protect the wearer if it seals properly against the face. Fit testing verifies that seal.
OSHA recognizes two types of fit testing. Qualitative fit testing (QLFT) uses the wearer’s sensory response to a test agent — either a bitter or sweet aerosol, or irritant smoke — to detect leakage around the facepiece. It’s the simpler and more common method for half-face respirators. Quantitative fit testing (QNFT) uses instrumentation to measure actual leakage by comparing particle concentration inside and outside the facepiece, and is required for full-face respirators in most applications.

Fit testing must be performed before initial use of a respirator, whenever a different respirator facepiece is used, and annually thereafter. It also needs to be repeated if the worker experiences significant changes in physical condition — weight loss, dental work, facial scarring — that might affect the seal.
Here’s what I see in training sessions more often than I’d like: workers who’ve been issued the same respirator model for years and assumed fit was fine because “it feels okay.” Comfort and fit are not the same thing. A respirator can feel perfectly wearable while channeling contaminated air around the seal with every breath. The fit test is the only way to actually verify protection — and it regularly reveals problems that would never have been caught otherwise.
Respirator Selection: Matching the Device to the Hazard
The standard requires that respirator selection be based on actual workplace hazards — not on what’s cheapest, what’s in the supply cabinet, or what workers seem most willing to wear. Employers are required to identify and evaluate the respiratory hazards in the workplace, including the nature of the hazard (particulate, gas, vapor, or combination), the concentration, and the oxygen content of the atmosphere.

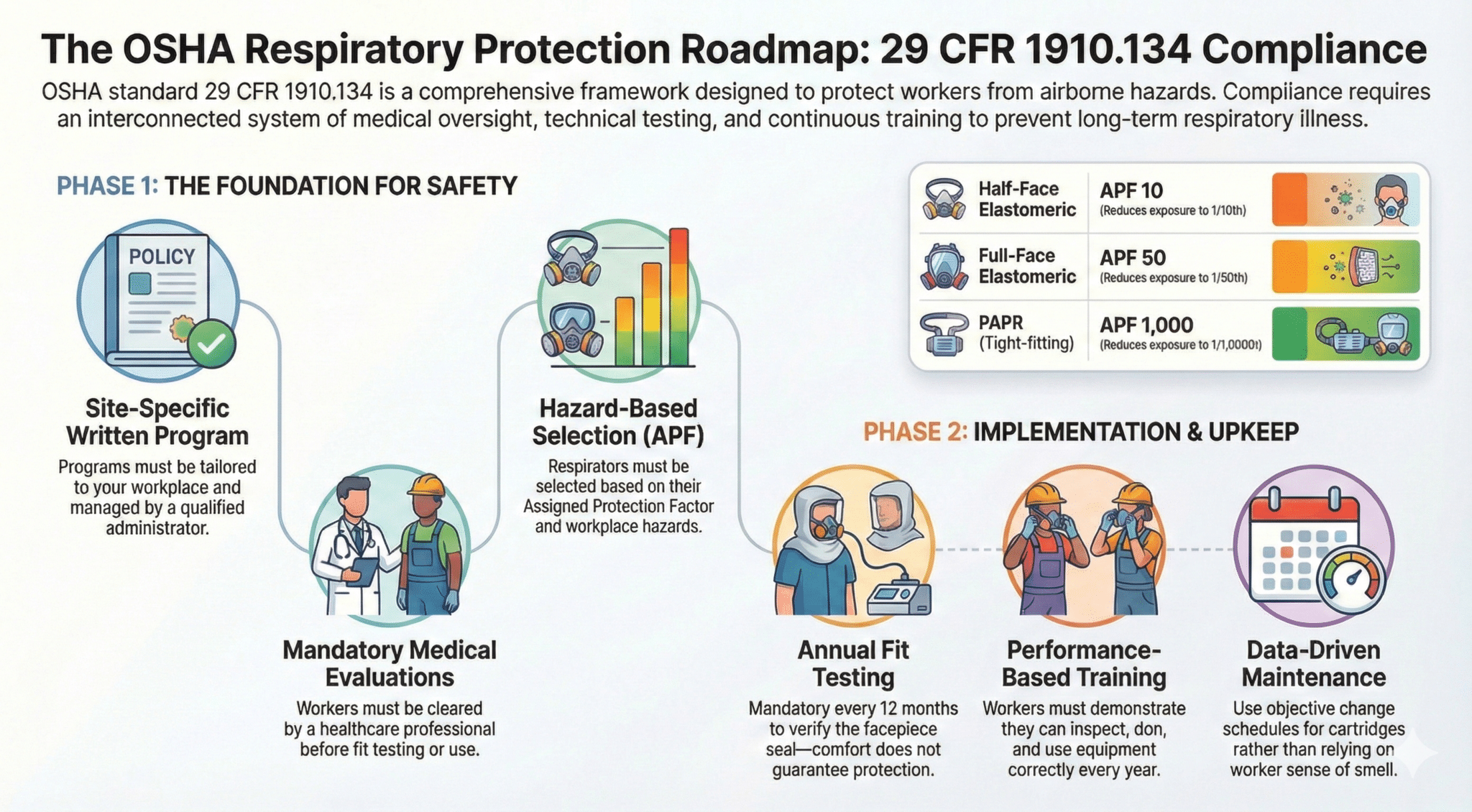
From there, respirator selection involves matching the device’s assigned protection factor (APF) to the actual exposure. The APF represents the minimum anticipated level of protection a properly functioning respirator provides when worn correctly. For a half-face elastomeric respirator, the APF is 10 — meaning it reduces exposure to 1/10th of the surrounding concentration. A full-face respirator has an APF of 50. Powered air-purifying respirators (PAPRs) with tight-fitting facepieces reach an APF of 1,000.
If monitoring data shows that the airborne concentration of a contaminant exceeds the permissible exposure limit (PEL) by a factor of 25, a half-face respirator with an APF of 10 isn’t an adequate solution. The employer needs to either control the hazard at the source or select a respirator with a sufficient APF to bring the worker’s actual exposure below the PEL.
Training Requirements
Every worker required to use a respirator must be trained — and the training has to be comprehensive enough that they understand why they’re wearing the respirator, what it protects against, its limitations, how to put it on and take it off, and what to do if it becomes damaged or contaminated during use.
Training is required before initial use and annually thereafter. It also has to be repeated whenever there’s reason to believe a worker doesn’t understand the proper use, or when workplace conditions change in ways that make previous training obsolete.
In practice, what OSHA is looking for is that workers can demonstrate understanding, not just that they sat through a class. A signed attendance sheet isn’t training. I’ve worked with hotel engineering crews who could recite the donning procedure correctly in a classroom and then put on a half-face respirator backwards in the field because they’d never actually practiced it with their hands. Training has to bridge that gap.
Effective respiratory protection training covers: why respiratory protection is necessary for this specific job, the hazards the respirator protects against, the respirator’s limitations, how to inspect the respirator before each use, proper donning, doffing, and adjustment, how to recognize when the cartridge or filter needs to be replaced, fit check procedures, and proper storage and maintenance.
Maintenance, Cleaning, and Storage
Reusable respirators — half-face and full-face elastomerics, PAPRs, and supplied-air systems — must be cleaned, inspected, and maintained on a regular schedule. The standard specifies that respirators must be cleaned and disinfected as often as necessary to maintain sanitary condition, and that each worker assigned a respirator for regular use gets a unit that fits properly and is in good working condition.

Cartridges and filters have a finite service life. For chemical cartridges, service life depends on the concentration of the contaminant, the humidity, temperature, and work rate of the wearer. Employers are required to use either an end-of-service-life indicator (ESLI) or a change schedule based on objective data — you can’t simply tell workers to change their cartridges “when they smell something.” That approach leaves the hazard assessment in the hands of the worker’s nose, which is unreliable for many hazardous substances and simply doesn’t work for contaminants with poor odor warning properties.
Storage matters too. Respirators stored in dusty toolboxes, coiled hoses tossed into open bins, or facepieces left sitting on a workbench are going to degrade. The standard requires that respirators be stored in ways that protect them from damage, contamination, and environmental conditions that could compromise the facepiece or cartridges.
Recordkeeping
OSHA’s respiratory protection standard includes recordkeeping requirements. Specifically, employers must retain written records of medical evaluations (or at minimum the PLHCP’s written recommendations), fit test results, and training documentation.

Fit test records must be kept until the next fit test. Medical evaluation records must be retained for the duration of employment plus 30 years under OSHA’s medical records standard (29 CFR 1910.1020). Training documentation should be retained long enough to demonstrate compliance during an inspection.
Good recordkeeping also serves a practical function: it helps program administrators track when annual fit tests or training are due, identify workers who may need follow-up medical evaluations, and demonstrate due diligence if a worker later develops a respiratory illness.
Why the Whole Program Matters
The reason OSHA’s respiratory protection standard is structured the way it is — with all these interconnected elements — is that each piece fills a gap the others can’t cover. Medical evaluations catch health conditions that would make respirator use dangerous. Fit testing verifies the seal that training assumes is there. Training makes fit testing meaningful. Written programs make all of it consistent. No single element is sufficient on its own.
After years of delivering respiratory protection training to employees of all kinds, the message that tends to land hardest with workers is this: respiratory protection failures are often invisible until they’ve already done their damage. Lung disease doesn’t show up on the job. It shows up a decade later. The program requirements under 29 CFR 1910.134 exist specifically because those slow, invisible consequences are preventable with the right knowledge and the right equipment — applied consistently.